One of the most common questions I get when talking to new or prospective clients sounds a lot like this:
“What route of ketamine is best? I’ve read so much on the internet – one place says IV is best, and another website says the nasal spray is better. What gives!?”
The decision to pursue ketamine-assisted psychotherapy involves a significant investment of time and resources. Understandably, patients can feel confusion, anxiety, and pressure to pick the “right” or best treatment route.
So, which one?
The answer is simple: the “best” route for administering ketamine for treatment-resistant depression has not been established,1 meaning that there’s not one route of administration superior to another.
When thinking about what route is best for you, you should consider all factors, most importantly comfort, cost, and convenience. Providers like me should also share the decision-making process with you on why they have chosen a certain route.
If you’d like a more technical explanation, keep reading!
Bioavailability and Dosing
A provider will normally start by discussing bioavailability and dosing flexibility in conjunction with specific treatment goals and preferences.
Ketamine bioavailability is expressed as a percentage. It’s the percentage of ketamine that’s circulating in your body and is able to have an active effect2. Bioavailability can be influenced by a person’s age, sex, genetics, pre-existing medical conditions, metabolism, and/or administration technique.
Dosing is a measure of how much ketamine we’re giving. Dosing flexibility refers to how much we can adjust the dose up or down “on the fly” in the clinic.
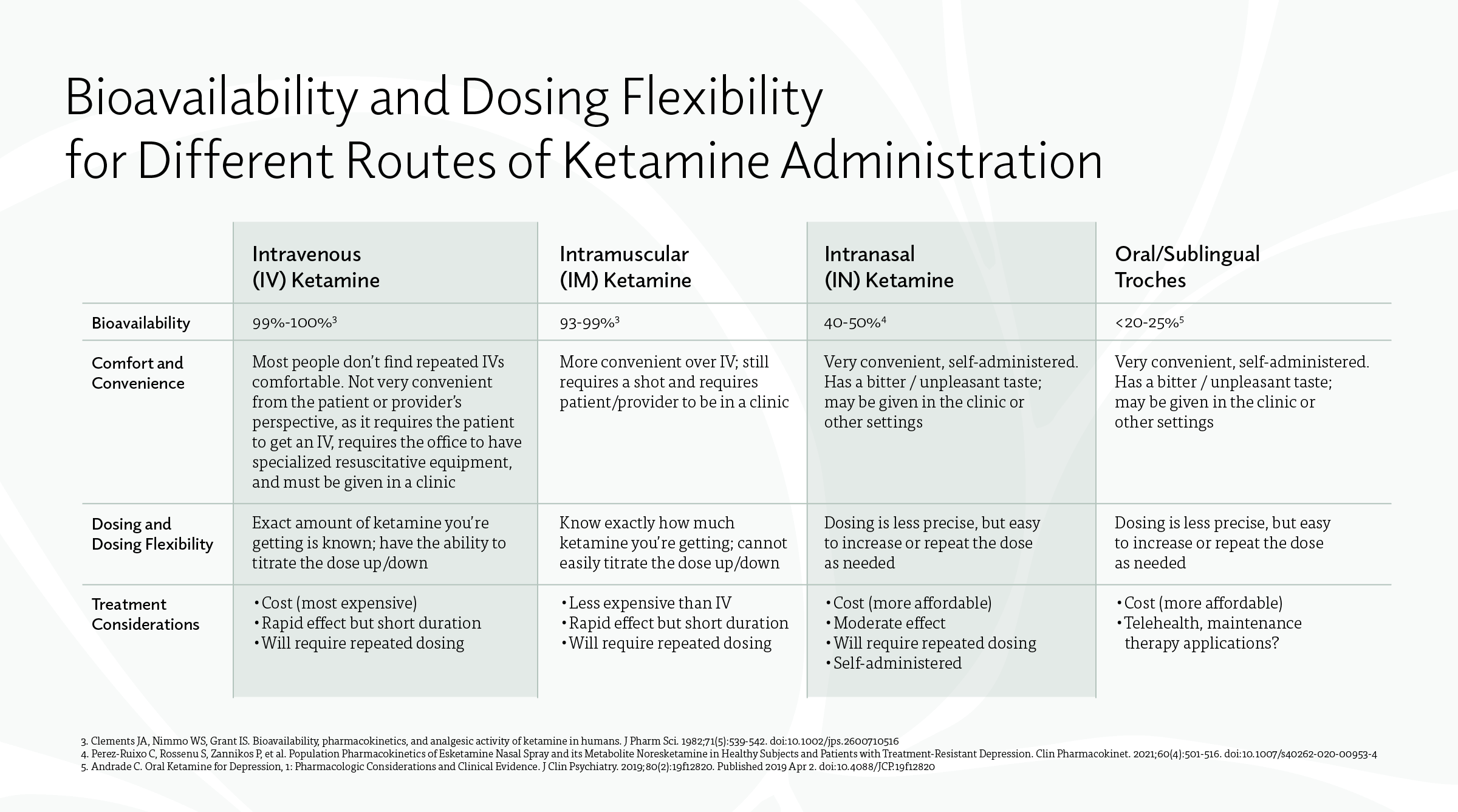
Check out the bioavailability and dosing flexibility comparisons between different routes of administration below:
Ketamine and Research
Many early research studies utilized intravenous (IV) ketamine. Because of this, many providers assume that IV ketamine is best because simply because it is the most researched. But it’s critical to remember that the researchers weren’t studying if IV ketamine was better than IM, IN, or oral forms of ketamine – they were trying to answer the bigger question first: is ketamine a safe and effective treatment for treatment-resistant depression?
IV ketamine is almost 100% bioavailable, making it a great choice for conducting a research study, because there’s likely to be less variability in how much of the drug is available between patients.
But for the individual, the choice isn’t as straightforward. The best route for you could be determined by a number of factors; it’s a decision that should be made between you and your provider.
So, what do you recommend?
I subscribe to the philosophy that it is less important how you get the ketamine into your body and more important what you do with it.
A single ketamine infusion can provide rapid relief from depressive symptoms, but the positive effects are not sustained beyond 4-7 days6.
Research has shown that there’s no benefit to giving bigger doses or loading doses (sometimes called an “IV push”). Repeated dosing is the only mechanism shown to sustain symptom relief.7
Psychotherapy works synergistically with ketamine to decrease cognitive distortions, improve neural plasticity, and stabilize synaptic connections in patients with severe major depressive disorder.8
REFERENCES
- Loo C. Can we confidently use ketamine as a clinical treatment for depression?. Lancet Psychiatry. 2018;5(1):11-12. doi:10.1016/S2215-0366(17)30480-7
- https://www.merckmanuals.com/professional/clinical-pharmacology/pharmacokinetics/drug-bioavailability
- Clements JA, Nimmo WS, Grant IS. Bioavailability, pharmacokinetics, and analgesic activity of ketamine in humans. J Pharm Sci. 1982;71(5):539-542. doi:10.1002/jps.2600710516
- Perez-Ruixo C, Rossenu S, Zannikos P, et al. Population Pharmacokinetics of Esketamine Nasal Spray and its Metabolite Noresketamine in Healthy Subjects and Patients with Treatment-Resistant Depression. Clin Pharmacokinet. 2021;60(4):501-516. doi:10.1007/s40262-020-00953-4
- Andrade C. Oral Ketamine for Depression, 1: Pharmacologic Considerations and Clinical Evidence. J Clin Psychiatry. 2019;80(2):19f12820. Published 2019 Apr 2. doi:10.4088/JCP.19f12820
- Ying Xu, Maree Hackett, Gregory Carter, Colleen Loo, Verònica Gálvez, Nick Glozier, Paul Glue, Kyle Lapidus, Alexander McGirr, Andrew A. Somogyi, Philip B. Mitchell, Anthony Rodgers, Effects of Low-Dose and Very Low-Dose Ketamine among Patients with Major Depression: a Systematic Review and Meta-Analysis, International Journal of Neuropsychopharmacology, Volume 19, Issue 4, April 2016.
- Zheng W, Zhou YL, Liu WJ, et al. Rapid and longer-term antidepressant effects of repeated-dose intravenous ketamine for patients with unipolar and bipolar depression. J Psychiatr Res. 2018;106:61-68. doi:10.1016/j.jpsychires.2018.09.013
- Wilkinson ST, Rhee TG, Joormann J, et al. Cognitive Behavioral Therapy to Sustain the Antidepressant Effects of Ketamine in Treatment-Resistant Depression: A Randomized Clinical Trial. Psychother Psychosom. 2021;90(5):318-327. doi:10.1159/000517074
| Intravenous (IV) ketamine | Intramuscular (IM) ketamine | Intranasal (IN) ketamine | Oral /sublingual troches | |
|---|---|---|---|---|
| Bioavailability | 99%-100%3 | 93%-99%3 | 40-50%4 | <20-25%5 |
| Comfort and Convenience | Most people don’t find getting repeated IVs comfortable. Not very convenient from the patient or provider’s perspective (requires the patient to get an IV, and requires the office to have specialized resuscitative equipment), must be given in a clinic | More convenient over IV; still requires a shot and requires patient/provider to be in a clinic | Very convenient, self-administered. Has a bitter / unpleasant taste; is usually administered in a clinic. | Very convenient, self-administered. Has a bitter / unpleasant taste; may be given in the clinic or other settings |
| Dosing and Dosing Flexibility | Exact amount of ketamine you’re getting is known, have the ability to titrate the dose up/down | Know exactly how much ketamine you’re getting, cannot easily titrate the dose up/down | Dosing is less precise, but easy to increase or repeat the dose as needed | Dosing is less precise, but easy to increase or repeat the dose as needed |
| Treatment considerations | Cost (most expensive) Rapid effect but short duration of effect Will require repeated dosing | Less expensive than IV Rapid effect but short duration of effect Will require repeated dosing | Less expensive than IV Rapid effect but short duration of effect Will require repeated dosing | Cost (more affordable) Moderate effect Will require repeated dosing Self-administered |




